
Genetics
In most individuals diagnosed with FTD (about 70–80%), there is no clear cause or family history of the condition. These cases are described as sporadic. FTD affects men and women roughly equally, and known risk factors are similar to those seen in other types of dementia.
Around 20–30% of individuals with FTD, however, have a genetic or familial form of the disease, meaning it runs in families and is caused by a change (mutation) in a specific gene. This is more common in some FTD syndromes than others.
In bvFTD, about 40% of individuals have a family history of the disease. In roughly half of these cases, a mutation is found in one of three known genes: MAPT, GRN, or C9ORF72. These mutations can be passed across generations. In other words, each child will have a 50% risk of inheriting the faulty copy of the gene from their affected parent.
In the language variants of FTD—SD and PNFA—a genetic cause is much less common, occurring in fewer than 5% of cases.
The combined presentation of FTD and MND has one of the strongest genetic associations. A C9ORF72 mutation is found in a high proportion of familial cases, and may also be present in individuals with no known family history, particularly if both cognitive and motor symptoms are present.
In families where no known mutation is found, other genetic factors may be involved but are not yet understood.
If you have a family history of FTD or concerns about inherited risk, speak with your treating clinician or contact our team to learn more about genetic counselling and testing.
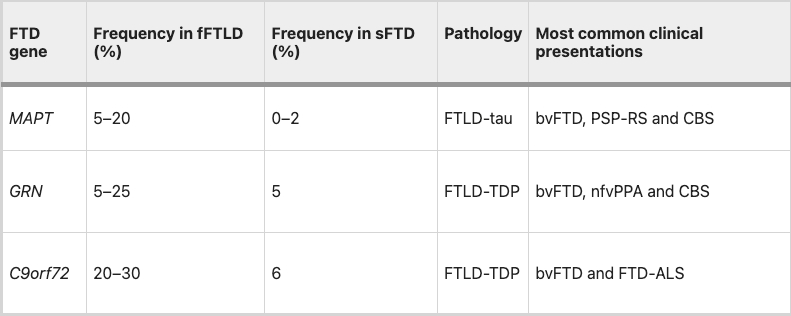
Frequency, pathology and common clinical presentations associated with FTLD are taken from Grossman, M., Seeley, W.W., Boxer, A.L. et al. Frontotemporal lobar degeneration. Nat Rev Dis Primers 9, 40 (2023). https://doi.org/10.1038/s41572-023-00447-0